What is it?
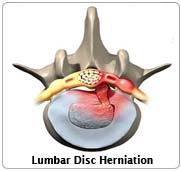
Your backbone, or spine, is made up of 24 bones (vertebrae), like a tower of hollow bricks held together by rubbery plates called discs. This arrangement helps you to bend your back. The central part of a disc is soft. This part has slipped out of place and is pressing on one of the nerves in your back. This makes you feel pain as if it is coming from your leg (sciatica). You may also have weakness in part of your leg. You may also have had, and still have, some back pain.
The Operation
 You will have a general anaesthetic, and will be asleep for the whole operation. A cut is made down to your backbone about three inches long, in your lower back. The soft part of the damaged disc is removed. This takes the pressure off the nerve in your back. The firm outer rim of the disc is not removed. The skin wound is then closed up with stitches or clips. You will be in hospital for one to three days after the operation. Previously a part of the vertebra, the lamina was always removed. The operation was therefore called a laminectomy. The operation is now either called a discectomy or a nerve root decompression.
You will have a general anaesthetic, and will be asleep for the whole operation. A cut is made down to your backbone about three inches long, in your lower back. The soft part of the damaged disc is removed. This takes the pressure off the nerve in your back. The firm outer rim of the disc is not removed. The skin wound is then closed up with stitches or clips. You will be in hospital for one to three days after the operation. Previously a part of the vertebra, the lamina was always removed. The operation was therefore called a laminectomy. The operation is now either called a discectomy or a nerve root decompression.
Any Alternatives
Physiotherapy, and all the usual measures have not helped. If you leave things as they are, the pain and weakness in your leg will probably remain as they are or even get worse. More scans or X-rays will not help.The aim of the operation is to cure your leg pain. Your back pain may remain unchanged after the operation. If your back pain is more of a problem than your leg pain, you should not have the operation. You should have the operation if:
- your leg pain is worse than your back pain
- you have had leg pain for several months and it is not getting better
- your leg pain is interfering with your life
- you have had a special scan that shows that you have a disc pressing on the nerve.
If you have all of the above you should have an operation.
Before the operation
Stop smoking and get your weight down if you are overweight. (See Healthy Living). If you know that you have problems with your blood pressure, your heart, or your lungs, ask your family doctor to check that these are under control. Check the hospital's advice about taking the Pill or hormone replacement therapy (HRT). Check you have a relative or friend who can come with you to the hospital, take you home, and look after you for the first week after the operation. Bring all your tablets and medicines with you to the hospital. On the ward, you may be checked for past illnesses and may have special tests, to make sure that you are well prepared and that you can have the operation as safely as possible.. Many hospitals now run special preadmission clinics, where you visit for an hour or two, a few weeks or so before the operation for these checks.
After - In Hospital
The wound may be painful. You will be given injections or tablets to control this. Ask for more if the pain is getting worse . A general anaesthetic will make you slow, clumsy and forgetful for about 24 hours. The nurses will help you with everything you need until you are able to do things for yourself. Do not make important decisions during that time. While you are in the hospital, you will gradually be able to get out of bed and be able to walk around the ward.
The discomfort of the operation can make it difficult to pass urine and empty the bladder. It is important that your bladder does not seize up completely. If you cannot get the urine flowing properly after six hours, contact the nurses or your doctor. The wound will have a simple adhesive dressing over it. The physiotherapist will teach you some exercises and give you advice. You may be advised to wear a corset for the few weeks after your operation.
Your stitches or clips are taken out 10 to 12 days or so after the operation. You will not need a dressing on the wound after that. Wash around the dressing for the first 10 days. You can wash the wound area as soon as the dressing has been removed and the stitches are out. Soap and warm tap water are entirely adequate. Salted water is not necessary. You can shower or take a bath as often as you like once the wound has healed. You will be given an appointment to visit the orthopaedic outpatient department six weeks or so after your operation. The nurses will advise about sick notes, certificates etc.
After - At Home
You should follow the advice given to you. Physiotherapy may be arranged. You should not drive for six weeks. Until three months after your operation you should not drive for longer than half an hour at a time. If your job entails mainly walking with no lifting, you may return to work after four weeks. If you mainly sit at work, you may return after six weeks. If your job involves heavy work or a lot of driving, you may return to lighter duties after 12 weeks. If your job involves very heavy manual work, you may have to think of changing it to a lighter job. You may swim six weeks after your operation. You may restart non-contact sports three months after your operation. When you start playing, you will not be able to play for as long as normal and your back will ache at the end of a game. If all goes well your leg pain should be reduced after your operation. Do not be tempted to do too much too soon. Your back will continue to improve for up to one year.
Possible Complications
As with any operation under general anaesthetic there is a very small risk of complications related to your heart or your lungs. The tests that you will have before the operation will make sure that you can have the operation in the safest possible way and will bring the risk for such complications very close to zero.
The nerve that the disc is pressing upon may be bruised during the operation. This temporarily stops it working, making part of your leg numb and slightly weak. It is very rare (1 in 1000 cases) for the nerve to be permanently damaged. There is a 1 in 10,000 chance of bowel or bladder incontinence after this operation. Wound infection sometimes happens. You will be given antibiotics to try and prevent this. Many people fear that if the surgeon's knife slips, they might be paralysed. This complication is extremely rare, almost not existent with modern orthopaedic surgery.
Advanced Reproductive Technology
- In Vitro Fertilisation (IVF)
- Intracytoplasmic Sperm Injection (ICSI)
- Donor egg and embryo programs
- In Vitro Fertilisation (IVF)
- Pre-implantation genetic diagnosis (PGD)
- Surrogacy programs
Dental Videos