What is it?
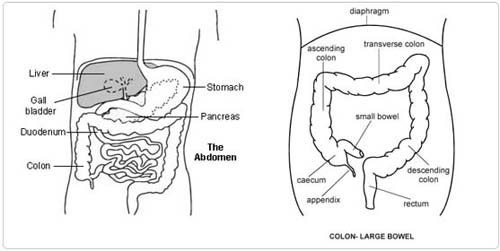
The bowel is a tube of intestine which runs from the stomach to the back passage. It is much longer than the inside of your belly (tummy). It fits in by coiling up in loops. The upper part of the bowel is called the small bowel. It joins the lower part of the bowel (the colon) just to the right of the waistline. This is where the appendix pouches out from the colon. The colon runs up to the right ribs and loops across the upper part of the belly. Then it passes down the left side to run backwards into the pelvis towards the back passage, where it is called the rectum. If most of the colon is diseased it can cause diarrhoea, bleeding or general illness. It is better removed. Sometimes the ends can be joined up inside your tummy. More often, the back passage is not healthy enough to make a safe join. Then the lowest part of the small bowel is brought out as a sort of spout (ileostomy) on the right side of the tummy. The bowel waste runs into a special bag stuck over the ileostomy.
The Operation
You will have a general anaesthetic, and will be asleep for the whole operation. A cut is made in the skin 25 cm (10 inches) long. The colon is freed inside your tummy. The diseased bowel is taken out. The lower end of remaining bowel is stitched shut. The upper end is made to open as an ileostomy. The wound in the tummy is stitched up. You should plan to leave hospital 2 weeks or so after the operation.
Any Alternatives
Leaving things as they are is risky. Bleeding or perforation mean that urgent operation is a must. General ill health will not get better by carrying on with drug treatment alone. A bigger operation to take out the back passage as well as the rest of the colon is not needed. There are three ways of dealing with the stoma. The simplest and most reliable is called a spout stoma, which the doctors are planning. This means wearing a bag to collect the waste. A second way is to make a pouch out of the bowel inside your tummy so that you can empty the pouch from time to time and there is no need to wear a bag. A third way is to make a pouch joined to the back passage so that the waste will pass out the normal way. The second and third operations are under development and can give rise to problems. Both the last two operations can be done on a spout stoma at a later date.
Before the operation
Stop smoking and try to get your weight down if you are overweight. If you know that you have problems with your blood pressure, your heart, or your lungs, ask your family doctor to check that these are under control. Check the hospital's advice about taking the pill or hormone replacement therapy (HRT). Check you have a relative or friend who can come with you to hospital, take you home, and look after you for the first week after the operation. Sort out any tablets, medicines, inhalers that you are using. Keep them in their original boxes and packets. Bring them to hospital with you.
On the ward, you may be checked for past illnesses and may have special tests, ready for the operation. Please tell the nurses of any allergies to tablets, medicines or dressings. You will have the operation explained to you and will be asked to fill in an operation consent form. Many hospitals now run special preadmission clinics, where you visit for an hour or two, a few weeks or so before the operation for these checks.
After - In Hospital
You will have a drip tube in an arm vein connected to a plastic bag on a stand containing a salt solution or blood. You may have a fine plastic tube coming out of your nose and connected to another plastic bag to drain your stomach. Swallowing may be a little uncomfortable. You will have a dressing on your wound and a drainage tube nearby, connected to yet another plastic bag. You may have a fine rubber tube (catheter) passing into the bladder through the front passage. This lets the bladder stay empty and small during the operation and helps control your body fluids afterwards. A general anaesthetic will make you slow, clumsy and forgetful for about 24 hours. Do not make important decisions during that time.
You will be expected to get out of bed the day after operation despite the discomfort. You will not do the wound any harm, and the exercise is very helpful for you. The second day after operation you should be able to spend an hour or two out of bed. By the end of four days you should have little pain. The ileostomy may not work for a day or two. It is always runny. It does not smell. You will get special advice and help from the Stoma Nurses. Because of the drainage tube (catheter) in the bladder, passing urine is not a problem. Once you can walk about in reasonable comfort, the catheter is taken out.
You can take the dressing off after 48 hours. Usually there are stitches or clips in the skin. The wound may be held together underneath the skin and not need further attention. There may be some purple bruising around the wound which spreads downwards by gravity and fades to a yellow colour after 2 to 3 days. It is not important. There may be some swelling of the surrounding skin which also improves in 2 to 3 days. You can wash the wound area as soon as the dressing has been removed. Soap and warm tap water are entirely adequate. Salted water is not necessary. You can shower or bath as often as you want. You will be given an appointment to visit the Out Patient Department for a check up about one month after you leave hospital. The stoma nurse will arrange to visit you at home. The nurses will advise about sick notes, certificates etc. Arrnagments will be made to take out the stitches or clips.
After - At Home
You are likely to feel very tired and need rests 2 or 3 times a day for a month or more. You will gradually improve so that by the time 3 months has passed you will be able to return completely to your usual level of activity. You can drive as soon as you can make an emergency stop without discomfort in the wound, i.e. after about 3 weeks. You can restart sexual relations within 2 or 3 weeks when the wound is comfortable enough. Sometimes the operation affects the sex nerves. This will be discussed with you. You should be able to return to a light job after about 6 weeks and any heavy job within 12 weeks.
Possible Complications
Complications are unusual but are rapidly recognised and dealt with by the nursing and surgical staff. If you think that all is not well, please ask the nurses or doctors. Chest infections may arise, particularly in smokers. Do not smoke. Occasionally the bowel is slow to start working again. This requires patience. Your food and water intake will continue through your vein tubing. Sometimes there is some discharge from the drain by the wound. This stops given time. Wound infection is sometimes seen. This settles down with antibiotics in a week of two. Aches and twinges may be felt in the wound for up to 6 months. Occasionally there are numb patches in the skin around the wound which get better after 2 to 3 months. The stoma can sometimes swell, or shrink or irritate the skin. The Stoma Nurses will help you here.
Advanced Reproductive Technology
- In Vitro Fertilisation (IVF)
- Intracytoplasmic Sperm Injection (ICSI)
- Donor egg and embryo programs
- In Vitro Fertilisation (IVF)
- Pre-implantation genetic diagnosis (PGD)
- Surrogacy programs
Dental Videos