| Title *
|
:
|
 |
| First Name *
|
:
|
|
| Last Name *
|
:
|
|
| Age *
|
:
|
|
| Country *
|
:
|
|
| Postal Address
|
:
|
|
|
|
|
|
| Home Telephone *
|
:
|
|
|
|
|
(Include Country & Local Code) |
| Mobile Telephone
|
:
|
|
| E-mail Address *
|
:
|
|
| Confirm Email Address *
|
:
|
|
|
|
|
|
|
When is it most convenient to contact you? |
|
|
:
|
|
|
|
|
|
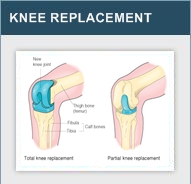
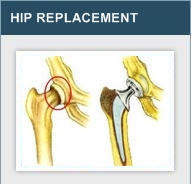
What type of treatment are you seeking information on? *
|
|
|
|
|
|
|
| Please specify *
|
:
|
|
|
|
|
|
| Please provide additional information that would help us assess your requirements *
|
|
|
|
|
|
|
|
i.) 'Do you suffer from conditions like BP, Diabetes, Hypertension OR Any other condition'
(Please answer in detail):
|
|
|
|
|
|
|
|
| ii.) Are you currently taking any medications (Please specify):
|
|
|
|
|
|
|
|
| iii.) Have you undergone any surgeries of late (Please specify):
|
|
|
|
|
|
|
|
| When would you like to have your treatment? (please specify month)
|
|
|
|
|
|
|
| Besides the treatment you are seeking, do you wish to have any other health consultations? |
|
|
Yes
No
|
|
|
|
|
| Would you like us to organise flights and accommodation for you? |
|
|
Yes
No
|
|
|
|
|
| Would you like us to organise visas for you? |
|
|
Yes
No
|
|
|
|
|
| Would you be accompanied by a relative or a friend? * |
|
|
Yes
No
|
|
|
|
|
| Where did you hear about us? * |
|
|
Internet
Magazine
FamilyOrFriend
Other
|
| What Hospital or Surgeon you would like to get your treatment from ?
|
|
|
|
|
|
|
| Do you have any other questions or comments?
|
|
|
|
|
|
|
|
|
|
|
| |
|
Agree to Terms and Conditions *
|
|
|
|
|
|
|